OIG Audit Intelligence
The Office of Inspector General audit wave has begun, and even well-intentioned providers are facing heightened scrutiny. For enterprise ABA providers and the PE firms backing them, the exposure is real, the timeline is now, and the path forward is operational.
Infographic
A one-page visual summary of the OIG audit wave: the data, the causes, and the operational priorities for enterprise ABA providers.
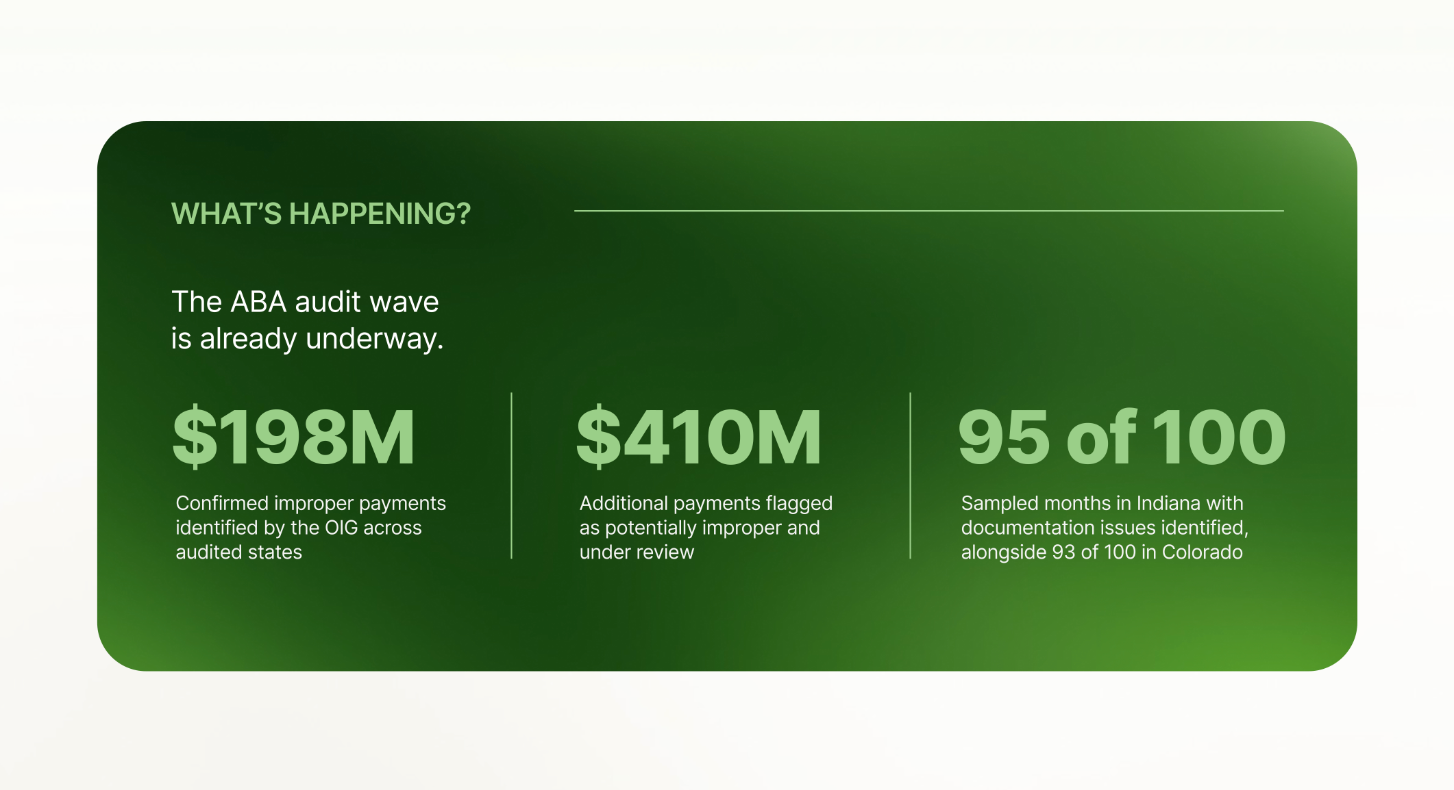
Download the infographicThe HHS Office of Inspector General is in the middle of a seven-state audit series on Medicaid-funded ABA services. Four states have been released so far, and each one shows the same general pattern: large volumes of questioned payments and widespread documentation issues across sampled claims.
ABA providers are receiving six-figure repayment demands for care they have already delivered. But what the OIG is actually finding is not usually fraud. In many cases, it is what happens when documentation standards were never clearly defined or consistently enforced.
What auditors are finding:
Late or incomplete session documentation. Missing or inconsistent timestamps. Supervision records not meeting timing requirements. Administrative errors in claim support documentation. Individually, these issues often reflect workflow or systems gaps rather than intentional misconduct. Collectively, they become material when assessed at scale across years of historical claims.
"In many cases, providers facing repayment demands delivered clinically appropriate care but operated within documentation systems that weren't fully aligned with payer or audit standards at the time."
Across all four states released so far, the OIG's recommendations are not primarily framed around fraud prevention. They largely point to the need for clearer, more consistent guidance on pre-payment standards for ABA services. Many of the claims under review date back years, sometimes as far back as 2019, and are being assessed against standards that were not always clearly defined or consistently understood at the time.
The numbers
Four states have been released so far. The pattern is consistent across each one.
None of this happened in a vacuum. 1 in 31 children in the U.S. are now diagnosed with Autism Spectrum Disorder. Demand was real and the industry responded. Commercial insurance expanded coverage first and Medicaid followed. Between 2019 and 2024, ABA visits on Medicaid grew 298% nationwide. States like Nebraska, Indiana, and Colorado saw spending balloon anywhere from 600% to 2,800% beyond original estimates. When a program grows that fast, the budget office notices.
The workforce scaled right alongside it. The BACB reports 253,397 RBT certificants as of April 2026, up from 89,122 in 2020, meaning more than half have entered the field in the last five years alone.
The infrastructure governing ABA billing never evolved at the same pace. Many Medicaid policies and billing frameworks were designed prior to this expansion and were not updated to reflect current volume, complexity, or workforce composition. That gap created an opening, and bad actors found it. Those cases represent a small slice of the market, and the scrutiny that followed impacts everyone.
The challenge is that most clinics were never built for this level of scrutiny. Clinics that scaled quickly to meet real demand are now being measured against documentation standards that they never fully understood and infrastructure that was never designed to support them.
The scale of growth
The industry scaled to meet real demand. But when Medicaid spending runs this far beyond estimates, budget offices notice and auditors follow.
The oversight wave is not slowing down. Operational standards for ABA providers will continue to evolve. Three enforcement escalations are already underway that will define the next phase of scrutiny.
House Committee on Energy and Commerce. Sent letters to ten states requesting information on Medicaid fraud, waste, and abuse, with ABA services specifically called out as high risk.
CMS CRUSH Initiative. Shifting from retrospective 'pay and chase' enforcement to real-time fraud detection across Medicaid programs.
Independent state action. Colorado, Indiana, Nebraska, New York, North Carolina, and Idaho have each taken action, from rate cuts and service caps to full service reclassifications.
"Audits are no longer a question. The question is whether your claims documentation holds up when one lands."
01. Conduct proactive internal audits. Find documentation gaps before external review does. The clinics that navigate this environment successfully are those that built operational infrastructure before scrutiny arrives, not in response to it.
02. Make documentation standards operational. Requirements should not exist solely in static manuals. They need to be integrated into day-to-day workflows, accessible at the point of care, and applied consistently across clinicians.
03. Understand claims performance across the full lifecycle. Pre-submission validation catches what auditors will find. Post-submission analysis tells you what historical exposure already exists. Most organizations are not consistently doing either.
By the time an audit letter arrives, the record already exists. Camber helps ABA providers validate claims before submission, giving teams a clearer way to catch documentation gaps, timing issues, and support errors before they become repayment risk.
For more background on the regulatory environment driving these audits, read our full analysis: Navigating a New Era of Oversight in ABA Spend.
Protect your claims
By the time an audit letter arrives, the record already exists. Talk to our team about how Camber validates claims before submission and reduces your exposure before auditors arrive.
Talk to our team{kind=link}